












HYPERTROPHIC CARDIOMYOPATHY
27 AUG 2010
HYPERTROPHIC CARDIOMYOPATHY
Sharmin Jahan Quader (PGFEM-2ND YEAR)
P K Prem Shankar Pandian (MEM- 1ST YEAR)
Fabith moideen V M Attending Emergency Physician
Venugopalan P P, HOD, Emergency medicine
A 65 yrs old man presented in ED at 2.30 am with
Symptoms
·Sudden onset breathing difficulty’
·Mild left sided chest pain for 2 hrs
·Generalized weakness for same duration
Allergies – Nil specific
Medications
·Clopidogrel 75mg 0-1-0
·Atorvastatin 10mg 0-0-1
Past medical history
·HTN – 10 yrs
·Dyslipidaemia – same duration
·Hypertrophic cardio myopathy – 5 yrs, on irregular follow up
Last meal – 9 pm, dinner
Event
·sudden onset dyspnea
·chest pain which woke up from sleep
Vitals
·Pulse – 68/min
·BP – 140/90 mmHg
·Temp – Normal
·SPO2 – 90% in room air.100% with 4L O2 by face mask
·GRBS – 127 mmol
Examination
·HEENT – JVP mildly elevated
·Cardiovascular System – pan systolic murmur
·Respiratory system – mild bilateral basal crepitation present, Bilateral air entry equal
·Gastrointestinal system – within normal limit
·Extrimities – mild bilateral pedal edema present
·Spine & back – within normal limit
·Nervous system – No focal deficit
Differentials
·Acute Coronary Syndrome
·Cardiogenic pulmonary edema
Investigations
·ECG

-LVH
-T inversion in lateral, anterior & inferior leads
-Incomplete LBBB
Chest X ray –
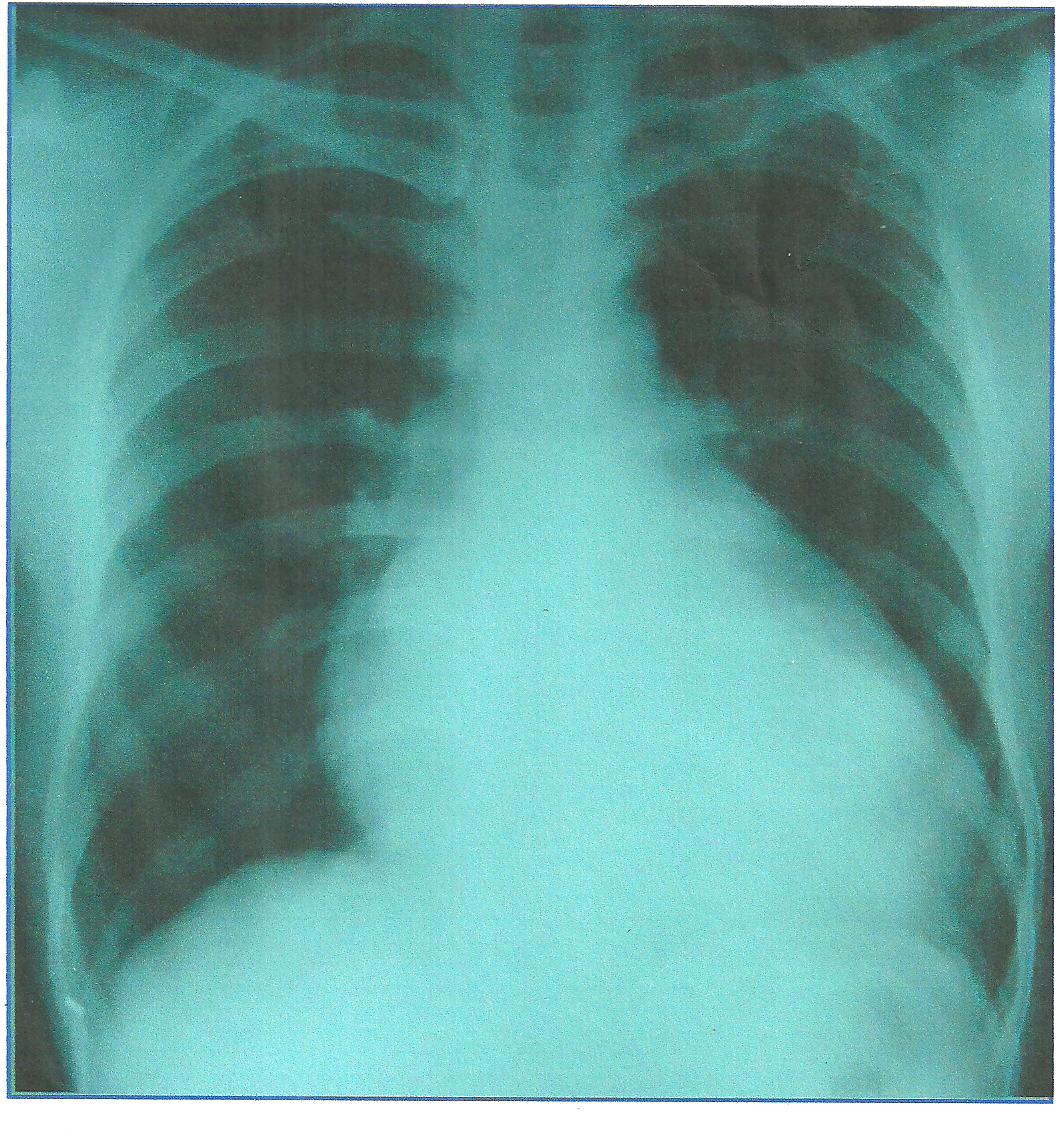
Cardiomegaly
§Lung fields – within normal limit
·TROP I – 0.06
·ECHO –
Apical HCM
-Mild MR, AS, AR
-Normal LV systolic function(EF-65%)
-LV diastolic dysfunction
·
Electrolytes – within normal limit
·
ABG – within normal limit
Cardiology consultation
Plan – conservative management with symptomatic treatment
HYPERTROPHIC CARDIOMYOPATHY
·Introduction –
Most common form of cardiomyopathy with prevalence of “100 per 10000”
·Definition – characterized by inappropriate and elaborate left ventricular hypertrophy with malalignment of myocardial fibre. The hypertrophy may be generalized or confined largely to the Interventricular septum, secondly a dynamic LV outflow tract pressure gradient, related to narrowing of the subaortic area
Clinical feature
·Mainly asymptomatic
·If symptomatic –
·Dyspnea
·Syncope
·Angina pectoris
·Fatigue
Physical examination
·Rapidly rising arterial pulse
·Hallmark of HCM – “Systolic murmur” usually begins after 1st heart sound (pansystolic due to mitral regurgitation)
·Murmur best heard at the lower left sternal border as well as apex
Evaluation
·ECG – Commonly LV hypertrophy & widespread deep broad Q waves
·ECHO – LV hypertrophy often with the septum ≥1.3 times the thickness of the LV free wall
Treatment
·Beta blocker & rate limiting Ca antagonist like Verapamil can help to reduce angina & syncopal attack
·Amiodarone for arrhythmia
·Partial surgical resection or septal ablation for improvement of outflow obstruction
·Implantation cardiac defibrillator(ICD) should consider in patients with clinical risk factors for sudden death
Precaution
·Digoxin & Vasodilators may increase outflow tract obstruction, hence should be avoided
Complication – sudden cardiac death
Risk factors for sudden death in HCM
·Recurrent syncope
·H/O previous cardiac arrest or sustained VT
·Exercise induced hypotension
·Marked increase in LV wall thickness
·Multiple episodes of sustained VT
Conclusion
Though not an immediate life threatening emergency, we should not take these patients casually as there is risk of sudden cardiac death. In ED we should evaluate these patients thoroughly in a proper way so that we can offer them a better chance of survival.
Bibliography
·TINTINALLI’S Emergency medicine,6TH ED
·DAVIDSON’S PRINCEPLES & PRACTICE OF MEDICINE, 20TH ED
·HUTCHISON’S CLINICAL METHODS,21ST ED
© Malabar Institute of Medical Sciences Ltd., All Rights Reserved

- Home
- About us
- Services
- Faculty
- Archives
- Articles
- Gallery
- Contact Us
- Website Design @ IPIX Solutions