












Sudden loss of vision
13 AUG 2010
SUDDEN LOSS OF VISION
AUTHORS:
Dr.Ramkumar S.[ MEM-PGY-1]
Dr.Abdul Jaleel P.M.[MEM-PGY-3]
Dr.Venugopalan P.P. [Chief-ED]
A 62 year old male presented to Emergency Department with
Symptoms: Sudden loss of vision both the eyes since morning
Vomiting 2 episodes
No pain on eye, No limb weakness or numbness
Allergies: None
Medications: None
Previous medical/surgical history: No significant co morbidities like hypertension, diabetes and convulsion.
O/E:
Airway : Patent
Breathing : Air entry bilaterally equal
respiratory rate-20/min
Circulation :Pulse-80/min,regular
BP-150/100 mmhg
Capillary refill-normal
Disability :Conscious, alert
Bilateral vision loss +
Bilateral pupils PEARL
Moving all four limbs
Exposure :No rashes or injuries
Vitals : Temp- 98.6 F
Pulse- 80/min
BP-150/100 mm hg
Respiratory rate- 20/min
GRBS- 101 mg/dl
Head to Toe Examination :
HEENT - Visual Acuity : Bilateral Eye no Perception of Light
- Occular Movements : Normal Bilateral
- Pupils : Normal Bilateral Eyes
- Funduscopy : Retina Normal Bilateral Eyes
-Disc & Vessels Normal Bilateral Eyes
No Pallor
No icterus
Neck : Trachea midline, no JVD
Chest : Air entry bilateral Equal,NVBS+
CVS : S1S2 +, No S3, No murmurs, No pericardial rub
P/A : Soft,no organomegaly
Extremities :Warm,No edema,pulses Normal
Spine & Back :Normal
Neurology : Conscious,Oriented, Normal speech
All cranial nerves normal
Motor, sensory all limbs normal
DTR, Plantar bilateral normal
No sign of meningeal irritation or cerebellar dysfunction
Differential Diagnosis :
Intra-cranial hemorrhage
Central Retinal Artery Occlusion
Central Retinal Vein Occlusion
Retinal detachment
Labs :
Hb- 13.4 mg/dl
WBC- 9700 /mm. cu.
Platelet-1.53 lakhs/mm. cu.
PT- 12.0
INR-1.0
RBC-4.27
ESR-15 mm/min
Na-133 mmol
K-3.2 mmol
ECG - Within Normal Limits
CT Brain(P): - Intracerebral bleed size 4.2cm * 2.8cm in the Rt. temporo-occipital lobe with
extension into Rt. lateral ventricle
- Mass effect with compression of occipital horn of Rt. lateral ventricle
- Hydrocephalus +
- Gliosis of Lt. occipital region with dialatation of Lt. lateral ventricle
- Bilateral ventricles are dialated
.jpg)
Neurology Consult-
IC bleed, de-edema measures, Neuro- ICU admission
Ophthalmologist Consultation :
- Visual Acuity : Bilateral Eye no Perception of Light
- Occular Movements : Normal Bilateral
- IOP : 17.3 Bilateral Eyes
- Pupils : Normal Bilateral Eyes
- Funduscopy : Retina Normal Bilateral Eyes
- Disc & Vessels Normal Bilateral Eyes
DIAGNOSIS: Intra-cerebral bleed Rt. temporo-occipital lobe with extension into Rt. lateral ventricles.
Patient admitted under Neurology in Medical ICU.
Treatment :
Anti hypertensives
Anti edema measures
Anti epileptics
Antibiotics
RT feeds
DISCUSSION:
Sudden loss of vision is classified as follows:
1. Painful & Painless
2. Unilateral & Bilateral
3. Acute & Progressive(Chronic)
Our Patient discussed above has a sudden loss of vision, the cause is intra-cerebral bleed. This not being a commonest cause. Acute vision loss usually occurs over a period ranging from a few seconds to a day or two. Most of these patients need Ophthalmic or Neurological referral for a complete workup.
Causes: Acute vision loss related to non- trauma is mainly due to
1. Vascular occlusion
2. Macular disorders
3. Neuro-ophthalomologic disease
4. Hysteria (Functional)
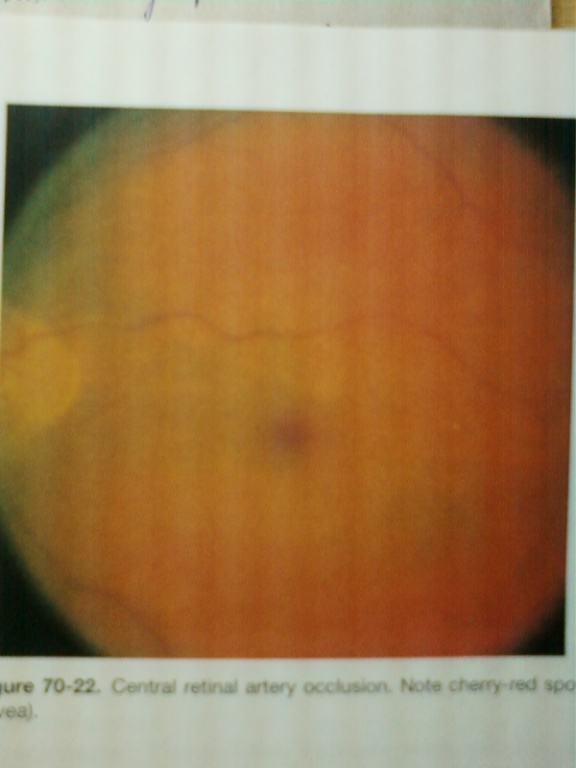
Central Retinal Artery Occlusion(CRAO) :
- Vision loss is painless
- CRAO causes an ischemic stroke of the retina
- Retina becomes pale, less transparent & edematous
- Funduscopy- "CHERRY RED SPOT"
Treatment:
- Digital orbital massage
- IOP reduced by Timolol Maleate 0.5%, Acetazolamide 500mg PO or IV
- Vasodialatation technique: Breathing into a paper bag for 5 - 10 min for increase in PaCO2
- Immediate Ophthalmic Consultation
- Complete medical evaluation (CRAO being an embolic event)
Central Retinal Vein Occlusion(CRVO):
- Vision loss is rapid & painless
- Thrombosis of central retinal vein
- Funduscopy: optic disc edema & retinal hemorrhages (blood & thunder fundus)

Treatment:
Tab. Aspirin 60-325 mg daily
Retinal breaks & detachments:
A retinal break is a tear in the retinal membranes may or may not lead to retinal detachments.
3 mechanisms
- Rhegmatogenous
- Exudative
- Traction
Ophthalmoscopy - Retinal detachment is seen (Out of focus at site of detachment)
Immediate Ophthalomology Consultation
Posterior Vitreous detachment:
- Seen in elderly
-With ageing vitreous gel pulls away from the retina
- Symptoms similar to Retinal detachment
Immediate Ophthalmic Consultation.
Vitreous Hemorrhage:
- Bleeding into the pre-retinal space or into the vitreous cavity
Causes:
- Diabetic retinopathy
- Retinal detachment
- Sickle cell disease
- Retinal artery micro aneurysms
- Trauma
Direct Ophthalmoscopy :
- Reddish haze in mild cases
- Black reflex in severe cases
Treatment :
- Treat underlying cause
Macular disorders :
- Loss of central vision & preservation of peripheral vision
- Most common degenerative maculopathy is Senile
Funduscopy :
- Scattered Drusens
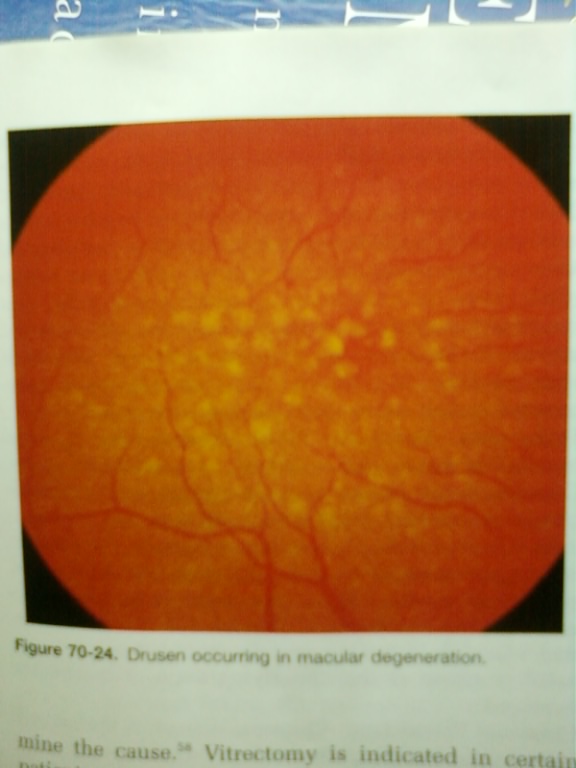
fig: Drusens are small sharply defined yellow-white masses
Treatment :
Photocoagulation as soon as possible.
Neuro-ophthalmologic visual loss :
No obvious abnormalities on physical examinations.
3 types: 1. Prechiasmal
2. Chiasmal
3. Postchiasmal
1. Prechiasmal:
- Decreased visual acuity or visual field loss unilateral or bilateral.
- Causes: a) Optic neuritis
b) Compressive optic neuritis
c) Ischemic optic Neuritis
d) Toxic optic neuritis
e) Metabolic optic neuritis
2. Chiasmal Visual loss:
- Chiasmal compression by Pituitary tumors, Craniopharingiomas, Meningiomas.
- Classical defect is bitemporal hemianopsia.
3. Post chiasmal visual loss:
- Causes are infarction, AV malformations, tumors & migraine.
- Visual defect is Homonymous hemianopia.
Fucntional (Hysterical) :
- Examinations to rule out possible neuro-ophthalmic deficits.
Conclusion
Bilateral sudden loss of vision , intracranial bleed should also be considered as a cause during the workup ,even if it is not so common.
References :
1. Rosen's Textbook of Emergency Medicine 6th edition.
2.Tinttinalli Emergency Medicine 6th edition.
3. Davidson’s Principles and practice of medicine 20th edition.
4.Parson's Disease of eye.
5.Medscape online reference.
© Malabar Institute of Medical Sciences Ltd., All Rights Reserved

- Home
- About us
- Services
- Faculty
- Archives
- Articles
- Gallery
- Contact Us
- Website Design @ IPIX Solutions